Menopause and joint pain go together more often than most women expect, and the knees tend to take the biggest hit. Falling oestrogen levels directly affect cartilage health, synovial fluid production, and joint inflammation. Research shows that more than 50% of women experience musculoskeletal symptoms during the menopause transition, with menopausal knee pain being among the most reported yet least discussed.
There is solid science behind why so many women in their 40s and 50s start noticing aching, stiff, or swollen knees around the time of menopause. The good news is that effective help exists at every stage, from targeted exercises and lifestyle changes to advanced clinical treatments like Arthrosamid injection.
What Is the Link Between Menopause and Joint Pain?
Menopause and joint pain share a common root: oestrogen.
When women enter perimenopause typically in their mid-40s oestrogen levels begin to fall. This hormone does far more than regulate the menstrual cycle. It actively protects joints by reducing inflammation, maintaining cartilage health, and keeping synovial fluid (the lubricant inside the knee joint) at healthy levels.
As oestrogen drops, these protective effects weaken. Inflammation rises. Cartilage starts to degrade faster. The knee joint, which bears full body weight with every step, becomes a prime target.
Studies suggest that more than 50% of women experience musculoskeletal symptoms during the menopause transition. Joint pain menopause often appears alongside other perimenopause symptoms UK women commonly report such as hot flushes, sleep disruption, and mood changes but it frequently goes unrecognised as a hormonal issue.
Is Knee Pain a Symptom of Menopause?
Many women visiting their GP for sore knees get sent for X-rays or referred to rheumatology. Tests for lupus, Lyme disease, and rheumatoid arthritis come back normal. Then someone finally asks: could this be menopause?
The answer, very often, is yes. Knee pain is absolutely a symptom of menopause and it is more common than most people realise.
The Role of Oestrogen in Knee Health
Oestrogen receptors exist throughout the musculoskeletal system, in cartilage, bone, ligaments, and tendons. This means oestrogen directly influences how these tissues function and repair themselves.
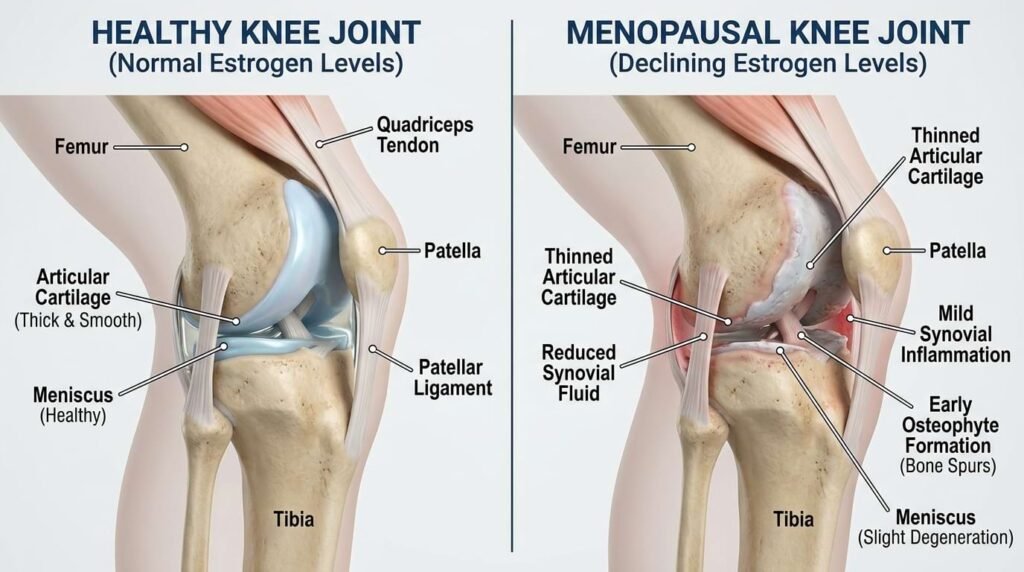
When oestrogen levels decline:

Cartilage becomes thinner and more susceptible to wear. The synovial membrane produces less lubricating fluid. Inflammation in the joint increases. Ligament laxity rises, making the knee less stable. Bone density decreases, raising the risk of fractures.
This combination creates the perfect storm for knee discomfort, especially in women who were already physically active or had a previous knee injury. Using a knee pain symptom checker at this stage can help identify whether the pain is structural, inflammatory, or hormonally driven.
How the Musculoskeletal Syndrome of Menopause Develops
The term musculoskeletal syndrome of menopause (MSM) is gaining recognition among specialists. It describes the cluster of bone, muscle, and joint changes that occur as oestrogen declines.
Estimates suggest that up to 70% of midlife women experience some form of MSM. It often starts subtly with a bit of morning stiffness, some discomfort when climbing stairs then gradually intensifies if left unaddressed.
Muscle mass also reduces during this period. Less muscle means less support around the knee joint, which adds further strain on already-stressed cartilage and ligaments.
Recognising Menopausal Knee Pain Symptoms
Not all knee pain feels the same. Knowing where and how the knee hurts can help women communicate symptoms more effectively with their doctor.
Knee Pain Inner Knee No Swelling
Pain on the inside of the knee with no visible swelling is a common presentation during menopause. This often points to early cartilage wear on the medial compartment of the knee. The joint feels achy and tender, especially after sitting for long periods or during low-impact movement. Many women dismiss this as “getting older” but it deserves proper assessment.
Lateral Knee Pain
Pain on the outer side of the knee known as lateral knee pain can indicate iliotibial band tightness or early osteoarthritis on the lateral compartment. During menopause, reduced muscle mass around the hip and thigh can alter knee alignment, making this type of pain more likely.
Knee Pain Walking Down Stairs
Knee pain walking down stairs (rather than up) usually points to the patellofemoral joint, the kneecap and the groove it sits in. Reduced oestrogen affects the cartilage behind the kneecap, and descending stairs places significant force on this area. Many women in perimenopause notice this as their very first symptom.
Can Menopause Cause Knee Swelling?
Yes, it can. Inflammation inside the joint called synovitis can cause visible swelling around the knee. When oestrogen drops, the anti-inflammatory protection it normally provides weakens, allowing low-grade inflammation to build up inside the joint capsule.
Not all menopausal knee pain involves swelling. Many women experience significant pain and stiffness with no outward sign at all. Both are valid, and both deserve attention.
How Long Does Menopause Joint Pain Last?
This is the question almost every woman asks and the honest answer is: it depends.
For some, joint discomfort eases within a year or two of entering full menopause, once hormone levels stabilise at their new baseline. For others, particularly those who develop underlying knee osteoarthritis as a result of hormonal changes, the pain becomes chronic and progressive.
The key variable is whether structural joint damage, cartilage loss, bone remodelling has already begun. If it has, the pain will not simply resolve on its own. It needs active management.
This is why acting early matters. The earlier menopausal knee pain is addressed, the better the chances of slowing down joint degeneration and maintaining quality of life.
How to Treat Joint Pain During Menopause
There is no single answer here. Treatment depends on how severe symptoms are, what is causing them, and how much they affect daily life. Most women benefit from a combination of approaches.
Exercises for Knee Pain Relief
Movement is medicine. Regular exercise is one of the most evidence-backed ways to reduce menopausal knee pain. Recommended exercises for knee pain include straight leg raises to strengthen the quadriceps without loading the joint, shallow wall squats to build thigh muscle support, step-ups to improve knee tracking and stability, swimming or aqua aerobics for full-body conditioning with minimal joint stress, and low-resistance cycling to maintain range of motion without impact.
A physiotherapist can design a programme specific to the individual’s knee anatomy and pain pattern.

Magnesium, Arthritis, and Joint Health
Magnesium plays a role in muscle function, nerve signalling, and bone mineral density. Research suggests that the relationship between magnesium and arthritis is worth exploring. Low magnesium levels are associated with higher inflammatory markers, which drive much of the joint pain during menopause.
Maintaining adequate levels through diet (leafy greens, nuts, seeds) or supplementation may support overall joint and muscle health during the menopause transition. A GP should be consulted before starting any supplement regimen.
Massage for Knee Pain
Massage for knee pain, particularly around the quadriceps, hamstrings, and IT band, can reduce muscle tension that contributes to abnormal knee loading. Sports massage and myofascial release techniques are especially useful for women experiencing lateral knee pain linked to tight outer thigh muscles.
Massage does not treat the underlying joint, but it can significantly reduce the muscular component of pain and improve the ability to exercise comfortably.
Hormone Replacement Therapy (HRT)
HRT replaces the oestrogen that menopause removes. Since oestrogen directly protects joint cartilage and reduces inflammation, it may help ease joint pain menopause triggers particularly for women in early menopause or perimenopause whose pain is primarily hormonal rather than structural.
HRT is not suitable for everyone. The decision should always be made in consultation with a GP or gynaecologist who can weigh up the full medical history and individual risk factors.
When Conservative Treatments Fall Short: Exploring Advanced Solutions
If lifestyle changes, physiotherapy, and HRT are not delivering enough relief, more targeted clinical treatments are worth exploring. This is especially relevant when knee osteoarthritis rather than pure hormonal pain has developed.
Stem Cell Treatment for Arthritis
Stem cell treatment for arthritis is an emerging area of regenerative medicine. The aim is to use the body’s own biological material to encourage cartilage repair and reduce inflammation in the joint.
Early results are promising, but the evidence base is still developing. Stem cell treatments are not yet widely available on the NHS and vary significantly in quality across private providers. Advice from a qualified orthopaedic specialist should always be sought before pursuing this route.
Arthrosamid Injection for Menopausal Knee Pain
For women with confirmed knee osteoarthritis whether triggered by menopause or worsened by it, Arthrosamid injection is one of the most clinically supported non-surgical options available in the UK.
What is it?
Arthrosamid is a CE-marked hydrogel injected directly into the knee joint. Once inside, it integrates with the synovial tissue and provides durable mechanical cushioning. Unlike steroid injections, which offer short-term anti-inflammatory relief, or hyaluronic acid, which breaks down over time, Arthrosamid is designed to remain in place, providing support for up to five years from a single injection.

How does it work? When oestrogen loss accelerates cartilage breakdown, the knee joint loses its natural cushioning. Arthrosamid works by physically restoring that cushioning inside the joint capsule, reducing friction and mechanical stress on the damaged cartilage. This makes it a meaningful option as a knee injection for menopause joint pain where structural damage is confirmed.
When Arthrosamid works well:
Women with mild to moderate knee osteoarthritis who have not found sufficient relief from physiotherapy, weight management, or other injections are typically the best candidates. Women who want to delay or avoid knee replacement surgery also benefit significantly. Post-menopausal women with cartilage loss and persistent menopausal knee pain despite HRT and exercise are another strong candidate group.
When Arthrosamid is not the right choice:
Arthrosamid is not suitable for severe bone-on-bone arthritis where knee replacement is the clinically appropriate option. It does not work for inflammatory arthritis such as rheumatoid arthritis. Women who experience purely hormonal joint pain with no structural cartilage damage are also unlikely to benefit from it, as the pain in those cases does not originate from the joint mechanics that Arthrosamid addresses.
What to expect:
A 30-minute outpatient procedure under local anaesthetic. Ultrasound-guided for precision placement. Most patients return home the same day. Noticeable improvement typically within 4 to 6 weeks. Results sustained for up to five years.
Book a consultation with Mr Syed Nadeem Abbas at KneePainClinic UK to find out whether Arthrosamid injection is the right fit.
Living Well With Menopausal Knee Pain
A diagnosis of menopausal knee pain does not mean an end to an active, fulfilling life. Many women manage their symptoms effectively and continue doing the things they love, with the right strategies in place.
Weight Management Reduces Knee Load
Every extra kilogram places roughly four kilograms of additional force on the knee joint. Even modest weight loss can produce significant pain reduction in joint pain menopause cases. A GP or dietitian can help set realistic targets.
Sleep Quality and Pain Perception
Poor sleep, already a common perimenopause symptom in the UK, lowers the body’s pain threshold. Addressing sleep disruption through HRT, sleep hygiene changes, or other support often improves how menopausal knee pain feels day to day.

Footwear and Knee Pain Walking Down Stairs
Supportive, well-cushioned shoes reduce the impact force reaching the knee joint. High heels and completely flat shoes both contribute to abnormal knee loading, making knee pain walking down stairs noticeably worse.
Pacing Activity to Prevent Flare-Ups
Sustained low-impact movement spread throughout the day is better than long rest periods followed by bursts of activity. Short walks or gentle cycling every 30 minutes can reduce stiffness significantly.
Anti-Inflammatory Nutrition for Joint Health
A diet rich in omega-3 fatty acids, leafy greens, and colourful vegetables helps dampen the inflammation that worsens joint pain during menopause. Research around magnesium and arthritis also suggests adequate magnesium intake may further support joint health at this stage.
Social Connection and Mental Wellbeing
Living with chronic knee pain affects mood and motivation. Staying connected with others and maintaining a sense of identity outside the pain both contribute to better long-term outcomes. Menopause is a transition, not a life sentence.
FAQ
Is knee pain a symptom of menopause?
Yes. Falling oestrogen reduces cartilage protection and increases joint inflammation. Knee stiffness in the morning, pain on stairs, or aching after rest are among the most common and most underrecognised signs.
How long does menopause joint pain last?
Purely hormonal pain may ease once hormone levels stabilize. If osteoarthritis has developed, ongoing management is needed. Early action produces better outcomes.
What exercises for knee pain work best during menopause?
Swimming, cycling, straight leg raises, and shallow squats are well-suited to this stage of life. A physiotherapist should guide any new programme.
When does Arthrosamid injection help menopausal knee pain?
It works best for mild to moderate knee osteoarthritis with confirmed cartilage loss. It is not suitable for purely hormonal joint pain without structural damage, or for severe bone-on-bone arthritis.
Can menopause cause knee swelling?
Yes. Oestrogen decline weakens the joint’s anti-inflammatory defences, allowing low-grade inflammation to build up and sometimes cause visible swelling.
Is there a link between magnesium and arthritis?
Adequate intake through diet may support joint health, though it does not replace medical treatment.
Menopause and joint pain are closely connected, but they do not have to define how women live. With the right combination of exercise, nutrition, and clinical support, menopausal knee pain becomes something that can be managed not just endured. The earlier the right steps are taken, the better the long-term outcome. Whether that means targeted exercises, HRT, or a non-surgical option like Arthrosamid injection, effective help exists. A specialist consultation is always the best starting point.
Read more: Best Knee Pain Relief Foods to Improve Mobility and Joint Health
Read more: How Vitamins and Joint Pain Are Connected: A Complete Guide
Read more: What Happens If Knee Pain Is Left Untreated